by Mary Smith, PE, Senior Vice President
Hospitals and medical facilities are seeking surge space to accommodate a variety of functions during the current coronavirus (COVID-19) pandemic. Many have existing parking garages that could be considered for some of these needs.
Drive-through screening of symptoms and/or testing for viruses are viable options for existing parking structures that can maintain social distancing and reduce contagion, yet allow for significantly increased screening and testing in a community. These operations could be implemented in many parking facilities following proper evaluation of functional requirements.
Providing other services in parking structures or lots, including the full assessment and treatment done in an Emergency Department (ED) and/or non-acute isolation wards, is far more complicated and will be discussed in a separate article.
Drive-through Screening
On March 9, 2020 the U.S. Centers for Medicare and Medicaid Services directed that Medicare-participating hospitals with emergency departments provide a federally required medical screening examination to every patient that comes to an ED, including those suspected of having COVID-19. Hospitals are very concerned with reducing, if not eliminating, the presence of persons with COVID-19 from ED waiting rooms. Persons who are concerned they may have the virus, but do not have a family physician or are seeking screening outside of office hours may be screened without leaving their car. Medical personnel in protective gear ask the typical screening questions, take temperatures and measure blood oxygen. They can then refer patients for testing, to go home and quarantine, or go to the ER or a pop-up clinic for flu-like illnesses for further evaluation and treatment.
Drive-through Testing
Most testing centers currently require that the patient have an appointment (after being screened for meeting the testing criteria online or on the phone) and require an order from a doctor to perform the testing. For example, at least one location in Indianapolis is limited to doctors, nurses and first responders who do not meet the screening requirements at medical centers for rapid-results testing of patients; they still must have a doctor’s order and be screened online prior to testing at a drive-through.
Another option now being rolled out is drive-through testing, where medical personnel collect samples using nasal swabs to test for the COVID-19 virus. Note that blood testing of antibodies and other concerns is not included in this option. Faster processing of testing may be provided by medical centers with in-house labs within a matter of hours; typically, the results from drive-through testing are returned in several days and intended for cases that can be quarantined at home.
When screened (online or via phone), symptoms and recent travel history screening is performed and if the patient qualifies for testing, all the paperwork, including insurance information is gathered, e-signed by the patient and a code or PIN for identification at the test site provided for on-site processing. In smaller operations, the appointment may only be checked off a paper list of reservations.
In a small-volume-system with only a couple testing points, the swab sample “test tube” that is sent to a lab can already have the patient’s name and ID ready upon arrival to the testing facility. Another minute may be added if the staff member needs to apply ID information on the test tube. This type of screening can have an average service time of 2 minutes. (As a rapidly emerging service, there is little data on service rates available, and only minimal confirmation of average times has been performed for this paper.)
One report is that the average time for medical consultation with both screening and testing occurs at the test position is 12 minutes, a resulting net add of about 10 minutes for screening, plus 2 minutes for the nasal swab collection itself. As screening and testing expand, there may be no further need for appointments with screening on-site that requires more time and more space for queueing of vehicles for tests.
Currently, a checkpoint is required by Centers for Disease Control (CDC) for access to the queues and/or testing position. At this checkpoint, the patient may be advised to call or text the attendant with the PIN number for confirmation and the attendant would also visually check an ID such as a driver’s license photo. Other locations may be advised by signs as well as a bullhorn to display the ID, doctor’s order and proof-of-insurance to the checkpoint attendant through the window. Photos may be taken of these items on a smart phone device. If windows are kept up for this process, the checkpoint attendants would not require full Personal Protective Equipment (PPE), which are in short supply as of this writing.
The service time at the checkpoint can vary from about 10 seconds with PIN and ID verification to about 1 minute for visual verification and photos. Therefore, the service rate at the checkpoint can vary from about 360 vehicles per hour down to about 60 vehicles per hour per lane. Obviously, setting up a PIN verification with only visual ID confirmation is ideal. The driver is then advised to proceed to queue and/or to a testing position by a traffic director. The process for an appointment-only test with prior online screening is that after receiving an appointment for a test, the website will tell the patient to have their ID, and in some cases, a doctor’s order and proof-of-insurance ready before arriving. Signs on arrival advise the patients to keep their windows up and have the paperwork ready.
It is noted that there may be multiple patients in one car. While the service time at the testing spot is roughly the same for each patient tested, there are less cars in queue. Further, even if there is only one patient, it may be a passenger not a driver. We therefore have assumed that testing has one patient per car to be conservative for planning purposes.
If a testing location converts to a system where appointments are not required, and anyone can be tested, screening and patient information must be gathered at the testing site. We have assumed that the checkpoint attendant will hand the patient the paperwork to be filled out and signed while the vehicle is in queue. When the patient is ready to be tested, the vehicle would be directed to the testing location where paperwork is reviewed and accepted. The tester will first confirm that the patient does need immediate care and be directed to an ER where faster testing and more complete evaluation can be provided. A temperature may be taken for the record as well. The patient info also has to be added to the sample “test tube”. It has been reported that the service time at the testing location could increase to an average of 12 minutes if screening is added to the testing function.
Design Considerations
As long as the vehicles are personal passenger vehicles (cars, SUVs, pickups and passenger vans) and are accommodated in the overhead clearance of the parking structure, there should be no building code issues with this use. Typically, newer structures will have 7’0″ clear height which can accommodate all “light” passenger vehicles (as defined by the USDOT) manufactured in the US that have not been modified with roof racks or equipment. (An exception is the Sprinter Van, which is generally used for either commercial purposes or for paratransit). Most vehicles with roof top equipment can be accommodated in the 8’2″ minimum clearance required for van accessible spaces by the Americans with Disabilities Act (ADA). Some older garages may only have 6′ to 7′ clearance, which may require height screening outside the facility.
Screening and testing should also not occur on ramps between parking levels because the slope will be more physically taxing for staff. We suggest that queuing can occur on parking ramps, but do not recommend using express ramps with more than 6.5% slope for queuing, as the starting and stopping on steeper slopes can increase the stress and frustration of sitting in queue.
The selection of areas for screening/testing and queuing should also consider whether there is adequate natural ventilation for those functions, as vehicles idling can produce carbon dioxide (CO2) and other noxious gases including volatile organic compounds (VOCs), carbon monoxide (CO) and oxides of nitrogen (NOX). Therefore, conducting screening and testing in underground, enclosed and other areas of parking structures that do not have cross ventilation should be avoided. Adding large commercial fans may be appropriate even in above grade, open parking structures, given the number of staff members now working at drive-through testing and screening operations.
The functional considerations include:
- Isolating the testing zone with a vehicular path of travel from the vehicle entry to the testing queues, the queue area, and back to an exit. Most locations have been set up quickly and employ a significant number of traffic cones. Ideally this would be outside the normal parking access and revenue controls; if not a “grace time” for free parking may need to be added to the control system.
- The CDC also requires a rejection path for those that don’t have appointments, a doctor’s order or otherwise don’t meet the then-current testing criteria.
A parking structure with at least one “flat” bay for testing with a second adjacent bay for queueing could be converted to a drive-thru testing center. Based on a typical 60′ parking module with 90-degree parking, we would recommend a single center island between two rows of sawtooth testing where personnel would have the testing equipment on the center island. The sawtooth allows the vehicles to pull in and out more easily around the other vehicles than parallel parking; a person directing traffic can assign vehicles to a sawtooth position in a larger system.
The sawtooth spots on one side of the island naturally serve testing of passengers in cars, while the other serves the testing persons on the driver side. The sawtooth provides better protection for the staff who walk around the vehicle to test someone in the passenger seat. Further, in less busy hours, one person can perform the test for the two positions on either side of the island, alternating serving sides while the vehicles pull in and out. As an example, this two-sided operation is commonly provided at the toll plazas for parking at theme parks.
The sawtooth design keeps the equipment and supplies on a single centralized island that is 10 to 12 ft wide that maximizes operational efficiency in a 60′ or wider parking bay. If the parking structure has angled parking and less than a 60′ bay only one sawtooth on one side of an island may be accommodated. Another option is to use parallel parking testing points on both sides of a wide drive aisle (at least 20′ wide), but that requires two separate islands for equipment and supplies and staffing is less efficient.
An example of a very large, relatively high capacity operation is laid out below.
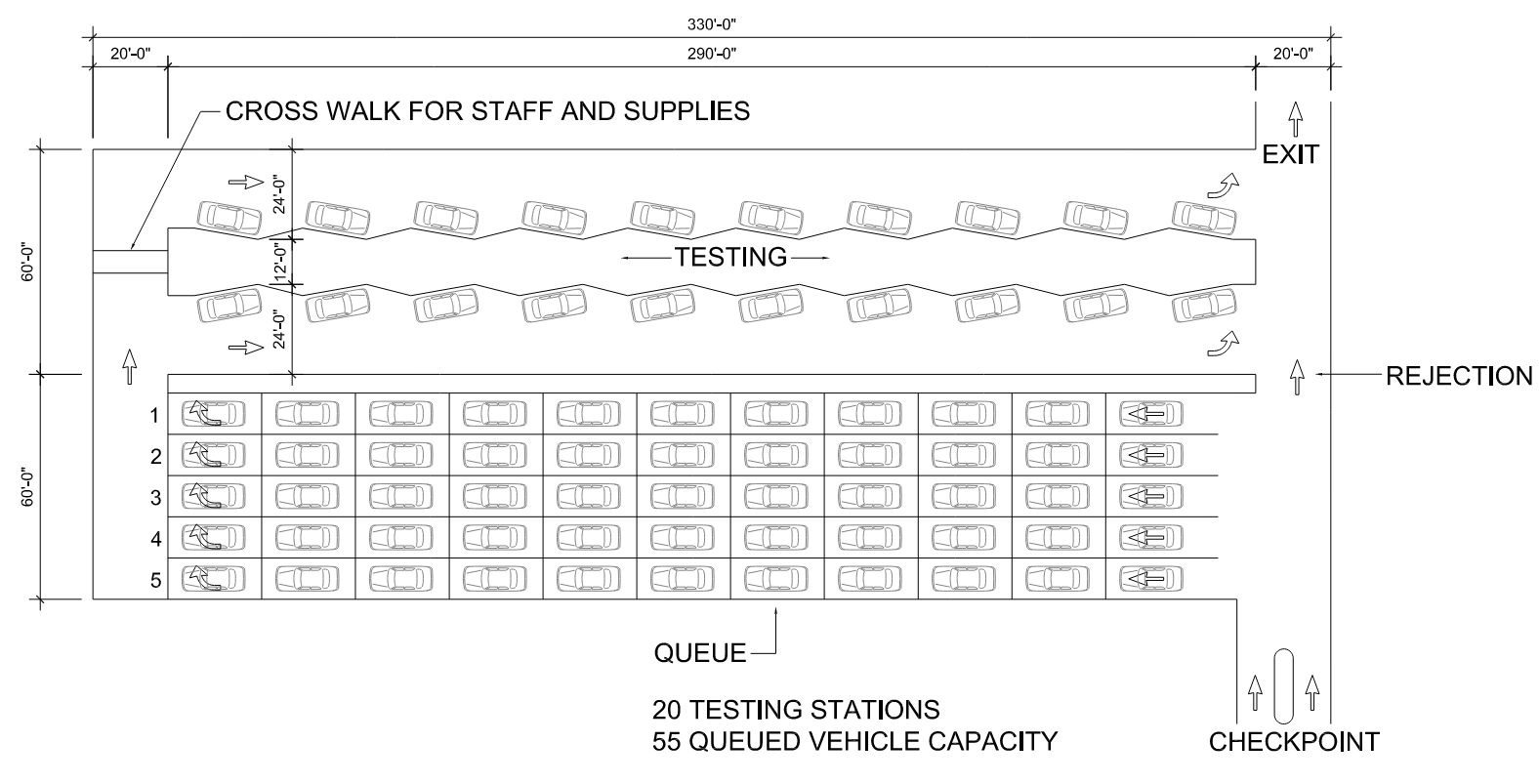
In a typical 330-foot-long parking structure bay, there will be 20 sawtooth spots, and 55 queued vehicles for testing. With an average 2-minute service time for prearranged appointments and all paperwork filed online, we would expect this layout to be able to process up to 30 vehicles per testing spot, 600 vehicles per hour (VPH). If screening is added to the process, the operation reduces to 5 VPH per testing spot and only 100 VPH maximum. It is obviously a very large operation in either case, with as many as 20 testers and 30 to 35 overall personnel in peak hours. Even though not required for an appointment-only operation, two lanes at the checkpoint would be advisable in the event that on-site screening is eventually added to the operation.
Once in the queue, the vehicles cannot bail out of the system in this design. A sign showing the average wait for testing should be placed before the checkpoint allowing the patient to opt to depart without testing. The queues would be loaded linearly. Rows 1 would be loaded with 11 cars, then 2 would be loaded with the next 11, then 3, 4, 5. The traffic director at the front of the queue would send each vehicle in line 1 to testing, before starting on line 2. Once the Row 1 vehicles have all been sent to testing spots and is empty, the traffic director at the checkpoint end would start refilling line 1 queue. This assures that the vehicles are served in a first-come, first-served order, even with multiple queue lanes.
This is similar to the operation at rental car return queues, or large taxi queue operations at airports. Alternatively, line 1 might be used for those with appointments and all paperwork filled online (aka express service), and the other queue lines used for those who require additional screening and other paperwork processing. In any event, this layout is far more space efficient than attempting to keep cars in a snaking, single queue line.
We have employed standard queuing theory to evaluate the queues and wait times. This theory assumes that the cars arrive randomly over the course of an hour (for example, an appointment for testing between 9 and 10 AM). For context, we have evaluated it for two options:
- No appointment required, with both screening and testing onsite, with an average service time at testing of 12 minutes and a 1-minute service time at the checkpoint
- Appointment-only testing with prior screening, and an average service time of 2 minutes at testing and 10 seconds at the checkpoint
There are obviously numerous variations in between those benchmarks which can be evaluated for a specific design. The predicted maximum queue is shown, with 90% confidence, along with the wait time at each point on the tables below. We also show those statistics for variations in operation with a lower volume that results in little or no queueing and one that is nearing capacity in a peak hour.
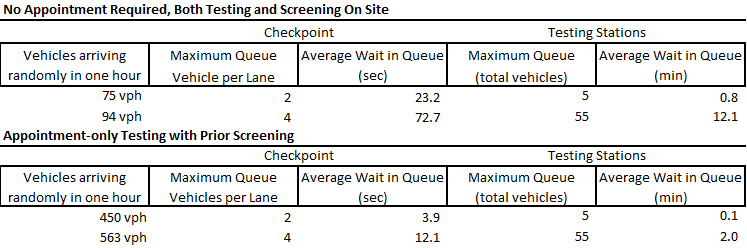
Note that although the nominal capacity is 100 VPH in the “no appointment required/with on-site screening” scenario, the queues approach infinity at 99 VPH. We set the volume to fill the queue space of 55 vehicles in this particular plan. Hypothetically, if 94 people are scheduled to arrive at 9:00 AM for prescreened appointment-only testing, the maximum queue would be 74 vehicles, the average wait would be 28.2 minutes and the last car in would wait 56.4 minutes. Therefore, testing centers should ideally schedule appointments in no more than 10- to 15-minute windows to minimize queueing at the start of each hour.
Conclusion
A significant testing and/or screening function can be implemented in existing parking structures with a reasonable level of attention to the functional and operational requirements of the proposed services. There is a large variation in queues and service times that would be based on the specific details of the operation. We have modeled what we consider to be two bookends for illumination of the issues and space requirements that might occur in a large system. Conversely, a much smaller operation could also be developed with only a few testing spots and much reduced queueing space required.
Questions?
Walker Consultants is an engineering and consulting firm with 23 locations around the nation. If you have questions regarding options at your parking facility, please contact Mary Smith.